
Review Article | DOI: https://doi.org/10.31579/2640-1045/055
1Division of Endocrinology and Metabolism, American University of Beirut
2Department of Internal Medicine, American University of Beirut
3Department of Anatomy, Cell Biology and Physiological Sciences, American University of Beirut
*Corresponding Author: Sami T. Azar, MD, Professor of Medicine, 3 Dag Hammarskjold Plaza, 8th New York, NY 10017, USA.
Citation: Rawaa El Sabbagh, Nadim S. Azar, Assaad A. Eid and Sami T. Azar (2021) Hypophysitis due to Immune Checkpoint Inhibitors J. Endo and Dis; 5(1); DOI:10.31579/2640-1045/055
Copyright: © 2021, Sami T. Azar, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 October 2020 | Accepted: 01 December 2020 | Published: 09 February 2021
Keywords: immune check point inhibitors, toxicity, endocrinopathy, CTLA-4 inhibitors, anti-PD1, anti-PDL1, hypophysitis
Immune checkpoint inhibitors are antineoplastic drugs associated with adverse events that result from unleashing the immune system against self-antigens while attacking neoplastic cells. Endocrinopathies are among the most common associated adverse events and hypophysitis is a frequent endocrine side effect of this treatment.
We conducted a systematic search of the literature in 2 databases: PubMed and Medline. Articles that reported endocrine adverse events of immune checkpoint inhibitors were reviewed.
Hypophysitis is most commonly seen with cytotoxic T-lymphocytes associated protein 4 (CTLA-4) inhibitors and can result in different anterior pituitary hormones deficiencies. Monitoring for this complication is of particular interest due to the life-threatening nature of secondary adrenal insufficiency and thyroid dysfunction if not promptly recognized and treated.
Hypophysitis is the most common endocrinopathy seen and is usually treated by adequate hormonal replacement. The use of high dose corticosteroids has not been established as a treatment of this endocrine toxicity. Hormonal screening should be a part of baseline laboratory testing of all patients undergoing treatment with immune checkpoint inhibitors.
Immune checkpoint inhibitors are new antineoplastic medications with expanding use in different types of cancer. The specific mechanism of action of these drugs results in a new type of adverse events related to the immune system [1]. Pituitary dysfunctions are among the most common adverse events observed. The increase in the use of immune checkpoint inhibitors and the improved survival of patients treated by these medications make the identification of endocrine side effects essential [1]. In fact, these endocrinopathies can affect the quality of life of the patients, and might be life-threatening in some cases if not promptly recognized and treated [1].
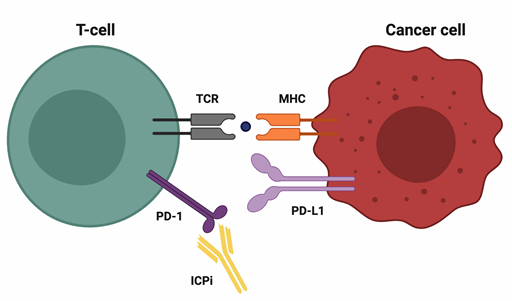
Over the past several years, the use of immune checkpoint inhibitors (ICPi) has changed the management and prognosis of many advanced solid tumors [1]. These drugs are monoclonal antibodies that block immune checkpoints that are present on the surface of T-cells to ensure immune self-tolerance, resulting in an increase of the T-cells ability to attack the cancer cells [2]. (Figure A and B).
Figure A: CTLA-4 pathway

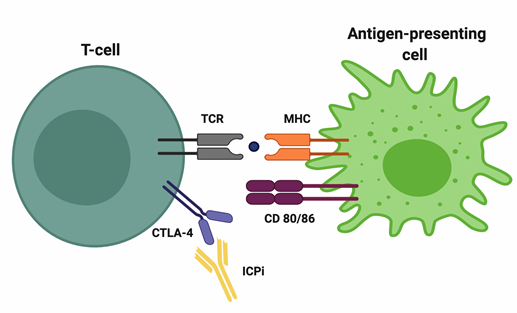
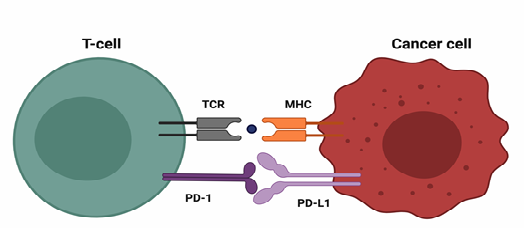
Figure B: PD-1- PD-L1 pathway
Currently, seven immune checkpoint inhibitors are approved for the treatment of different advanced solid tumors: a cytotoxic T-lymphocytes associated protein 4 (CTLA-4) inhibitor Ipilimumab; three programmed cell death protein (PD-1) inhibitors: Nivolumab, Pembrolizumab and Cemiplimab; and three programmed death-ligand 1 (PD-L1) inhibitors: Atezolizumab, Avelumab and Durvalumab [3-9]. Table 1 summarizes the different ICPi available and their various clinical indications.
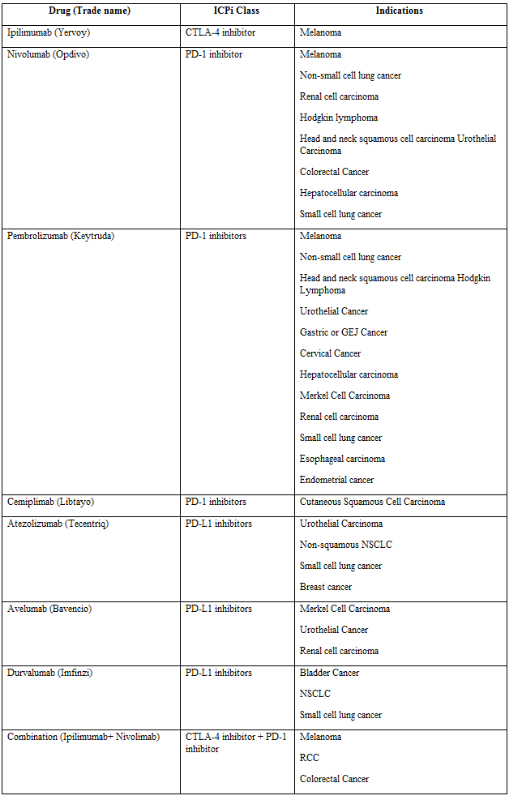
Abbreviations: GEJ: Gastro esophageal junction cancer, HCC: Hepatocellular carcinoma, HNSCC: Head and neck squamous cell carcinoma, NSCLC: Non-small cell lung cancer, RCC: Renal cell carcinoma, SCLC: Small cell lung cancer
ICPi are associated with immune related adverse events (IrAEs) that result from unleashing the immune system against self-antigens while attacking neoplastic cells [10]. Endocrinopathies are among the most common associated IrAEs, affecting the pituitary gland, the thyroid gland and to a lesser extent the pancreas, the adrenal gland and the parathyroid glands [11].
Search
We conducted a systematic search of the literature in 2 databases: PubMed and Medline. Articles that reported endocrine adverse events of immune checkpoint inhibitors were reviewed. We used the following keywords or corresponding Medical Subject Heading terms: “ipilimumab,” “nivolumab,” “pembrolizumab,” “atezolizumab,” “Cemiplimab” “Avelumab” “Durvalumab” “CTLA-4 inhibitors” “PD-1 inhibitors” “PDL-1 inhibitors” “immune checkpoint inhibitors” “endocrinopathies” “hypophysitis” “endocrine side effects”. We also reviewed references of published trials and review articles.
Pituitary dysfunction observed with ICPi is due to hypophysitis, which is the inflammation of the pituitary gland resulting in hormonal deficiency (12). Based on the results of a recent meta-analysis [13] the incidence of hypophysitis differs among ICPi regimens. It is higher with combination therapy (ipilimumab with nivolumab) reaching 8%. A lesser incidence is observed with CTLA-4 inhibitors monotherapy, estimated to be around 3.8%. Finally, the incidence of hypophysitis is very rare with PD-1 inhibitors (1.1%) [14]. The median time to onset of hypophysitis also varies depending on the molecule. It may occur early on in the setting of combination therapy (an average mean of 1 month), while with anti-CTLA-4 and anti-PD-1 therapy it may occur at 2-3 months and 3-5 months respectively [14, 15].
The pathogenesis of hypophysitis with ICPi is not clear. In a murine model of hypophysitis induced by ipilimumab, CTLA-4 was found to be expressed in pituitary cells, which could explain the higher incidence of hypophysitis with ipilimumab [16]. Some studies have shown that when ipilimumab binds to CTLA-4 on the pituitary cells, type II and type IV hypersensitivity reactions are induced, leading to hypophysitis [17, 18]. In one study, it was shown that antibodies against the anterior pituitary cells, namely the thyrotropic, corticotropic and gonadotropic cells, developed de novo in the serum of mice receiving the anti-CTLA-4 antibody [17]. This finding suggests that the humoral immune response may play a role in hypophysitis secondary to CTLA-4 inhibitors [17].
The symptoms of hypophysitis are not specific and depend on the affected pituitary axis, with headache being the most common symptom at presentation [17]. Secondary adrenal insufficiency is present in the majority of patients (91%) and can be differentiated from primary adrenal insufficiency (PAI) by the lack of hyperkaliemia or hypotension, while hyponatremia can be found in both conditions. Secondary hypothyroidism and hypogonadism are also common with an incidence reaching around 80% for each disorder. Patients with hypophysitis secondary to CTLA-4 inhibitors rarely present with diabetes insipidus, which can result in a loss of the posterior bright spots on T1-weighted MRI [19]. Growth hormone (GH) and prolactin deficiency are also very rare IrAEs [16]. Prolactin levels can be checked in those with secondary hypogonadism as hyperprolactinemia can result in hypogonadotropic hypogonadism. Prolactin may be either elevated or decreased in patients undergoing anti-CTLA4 therapy [20].
The diagnosis of hypophysitis due to immune checkpoint inhibitors is based on clinical, biochemical and/or radiological findings [21]. The workup should include free T4, TSH, cortisol level and an ACTH level ideally taken before starting steroids replacement. The measurement of gonadotropins is helpful in the diagnosis of pituitary insufficiency. However, the levels of gonadotropins and testosterone may be decreased in the setting of stress or with the administration of certain medications [22]. Because the treatment with GH analogs is contraindicated in the setting of active malignancy, GH screening is not recommended [23]. Magnetic resonance imaging (MRI) of the pituitary is the preferred imaging modality to make the diagnosis of hypophysitis and differentiate it from metastasis, infundibulo-hypophyistis, apoplexy and adenoma. In a recent review of case reports [19], in the majority of cases (108/222), imaging by MRI showed a mild to moderate enlargement of the pituitary gland. Normal MRI was found in 49 cases, pituitary atrophy was found in 3 cases and sella abnormality was seen in 3 cases. MRI was not reported/done in 22 cases. MRI may show thickening of the pituitary stalk [24] and sometimes heterogeneous gland enhancement on injection. Impingement of the optic chiasm is rarely seen, which explains the low incidence of visual disturbance in hypophysitis secondary to ICPi [16, 17, 18, 21, 23, and 24].
The management of hypophysitis requires hormonal replacement [25, 26]. In patients presenting with cardiovascular instability, adrenal crisis should be suspected and treated. Dexamethasone 4-10 mg should be used in cases where immediate blood withdrawal is not feasible before initiating steroids because dexamethasone does not ross react with cortisol in the radioimmunoassay. Once the patient is stable, the diagnosis can be confirmed by testing [27].
In central adrenal insufficiency, hydrocortisone replacement consists of daily doses of 15 to 20 mg, titrated to the patients’ clinical needs [28, 29]. Patients should be educated about sick day rules to increase their steroids dose and seek medical advice emergently [29]. In central hypothyroidism, thyroid hormone replacement can be initiated at low doses 0.8 mcg/kg/day and titrated gradually, according to free T4, due to the possible recovery of the thyroid axis [30, 31]. Glucocorticoid replacement should always precede thyroid replacement by days to avoid adrenal crisis precipitation [32].
The role of high dose glucocorticoids in the treatment of acute hypophysitis is highly debatable in the literature [33, 34, and 35]. Although it is recommended in the ipilimumab insert package [36]. In a retrospective study of 98 patients with hypophysitis due to ipilimumab, higher dose of glucocorticoids was associated with worse outcomes (shorter overall survival and time to treatment failure) compared with patients on replacement dose of steroids. This could be explained by the fact that high dose steroids might inhibit the effect of T lymphocytes and counteract the effect of immunotherapy [33].
The development of hypophysitis in the setting of ICPi use does not contraindicate the continuation of therapy. However, the decision to withhold it in the acute phase of hypophysitis depends on the severity of the symptoms [25].
The data available on the recovery of the pituitary gland after ICPi-induced hypophysitis is limited by the small sample size in most studies. Secondary adrenal insufficiency seems to be permanent in the majority of cases while secondary hypothyroidism and secondary hypogonadism have higher chances of recovery [33]. Patients with hypophysitis should be monitored closely, both clinically and biochemically, to adjust their hormonal replacement doses [25]. MRI of the pituitary gland after 3 months from the date of diagnosis is recommended by some guidelines in order to monitor pituitary inflammation and rule out the presence of metastasis [21].
Systematic hormonal screening before immunotherapy is not routinely recommended by all oncologic societies [25, 26]; however; it is recommended to keep a low threshold for pituitary hormonal testing in patients taking ipilimumab who present with non-specific symptoms. We recommend screening all patients undergoing ICPi therapy with TSH, FT4, 8 am serum cortisol, LH, FSH, testosterone/estradiol before the first immunotherapy course and at each immunotherapy infusion during the first 6 months. In asymptomatic patients with a normal hormonal workup, the frequency of hormonal monitoring can be decreased to every 2 months in the second 6 months of therapy and only in cases of suggestive symptoms thereafter [25, 26].
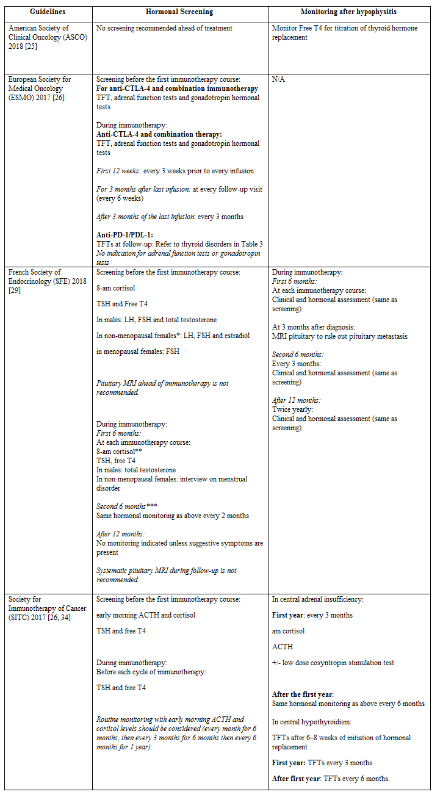
Abbreviations: FSH: Follicule stimulating hormone, LH: Luteinizing hormone, N/A: Not available, TFTs: Thyroid function tests
* in case of menstrual disorder
** in the absence of glucocorticoid drug treatment
*** If the patient is asymptomatic and hormonal work-up is normal
**** combination of anti-CTLA4 + anti-PD-1/PD-L1
ICPi therapy appears to play an important role in the development of hypophysitis. The pathogenesis of this mechanism, although incompletely elucidated, has been hypothesized to have different immunological mechanisms. Symptoms of hypophysitis induced by ICPi therapy are non-specific and mainly diagnosed on the basis of clinical, biochemical and radiologic findings. As for the management of hypophysitis, it consists mainly of hormone replacement. Different ICPi therapies work on different receptors and as such have a varied scale of ensuing physiological effects. Finally, different screening protocols and guidelines during and after immunotherapy are detailed.
The use of ICPi in different types of cancer is expected to increase in the upcoming years. This relatively new modality of treatment is challenging for all specialists, including endocrinologists, due to the unknown pattern of adverse effects. It is thus necessary to devise new studies regarding the therapy, in regards to pathophysiology, adverse reactions and treatment efficacy.
Abbreviations:
ACTH: Adrenocorticotrophic Hormone
Anti-TPO: Thyroid Peroxidase antibodies
Anti-ZnT8: Zinc Transporter Protein 8 antibodies
CTLA-4: Cytotoxic T-lymphocytes Associated Protein 4
DKA: Diabetic Ketoacidosis
DM: Diabetes Mellitus
GH: Growth Hormone
HbA1c: Hemoglobin A1c
ICPi: Immune Checkpoint Inhibitors
IrAEs: Immune Related Adverse Events
MRI: Magnetic Resonance Imaging
PAI: Primary Adrenal Insufficiency
PD-1: Programmed Cell Death Protein
PDL-1: Programmed Death-Ligand 1
PDL-2: Programmed Death-Ligand 2
TRAb: TSH Receptor Antibodies
TSH: Thyroid Stimulating Hormone
TFT: Thyroid Function Tests
Conflict of Interest
The authors of this review have no conflict of interest to disclose.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
